Flap Surgery for Breast Reconstruction
April 10, 2025
This page was reviewed under our medical and editorial policy by Antoine Carre, M.D., M.P.H., assistant clinical professor, Division of Plastic Surgery, Department of Surgery, and assistant clinical professor; and Susan Yost, Ph.D., staff scientist, Department of Medical Oncology & Therapeutics Research, City of Hope® Cancer Center Duarte
Not all patients choose to undergo breast reconstruction following breast cancer treatment. Patients who do will choose between using implants or undergoing flap (autologous) surgery. Flap surgery uses the patient’s own tissue to create a new breast.
For patients and families considering flap or autologous surgery, understanding the various types, procedures and benefits of each option may help them make a more confident, informed decision.
What Is Flap Surgery?
Flap surgery, also known as autologous tissue reconstruction or tissue-based reconstruction, is a type of breast surgery that rebuilds the shape of the breast after a mastectomy. This procedure uses tissue from other parts of the patient’s body, such as their back, abdomen, buttocks or thigh, to create a new breast.
One of the primary advantages of flap surgery over breast implants is that the reconstructed breast often looks and feels more like natural breast tissue. Additionally, since the tissue used is part of the patient’s body, it changes with weight fluctuations, providing a more natural appearance over time. Unlike breast implants, which may need to be replaced due to issues like ruptures, tissue flaps are durable and typically do not require replacement, reducing the need for future surgeries.
However, flap surgeries are more complex and involve a longer recovery period than implant-based reconstruction. This procedure requires surgery at both the patient donor tissue site and the breast site, leading to more scars and potential complications in two areas.
Flap surgery may be used alone or in combination with implants if additional volume is needed. This approach allows for a personalized reconstruction that aligns with the patient’s body and desired outcome.
Types of Breast Flap Surgery
In breast flap surgery, the surgeon removes a section of tissue, including skin, fat and sometimes muscle, from another site on the patient’s body. This donor tissue is then shaped to form a new breast and is either left attached to its original blood supply (pedicle flap) or is detached and reattached to a new blood supply in the chest (free flap).
Pedicle Flaps
Pedicle flaps are a type of breast reconstruction surgery used to rebuild the breast shape after a mastectomy. In this procedure, skin, fat and sometimes muscle are moved from one area of the body, such as the back or abdomen, to the breast.
The key feature of a pedicle flap is that the relocated tissue remains connected to its original blood supply. The patient’s donor tissue is tunneled under the skin to the breast area without the need to reconnect blood vessels, helping maintain blood flow to the transplanted tissue.
Free Flaps
Free flaps are a type of breast reconstruction surgery used to rebuild the breast shape after a mastectomy. In this procedure, tissue, including skin, fat and sometimes muscle, is completely detached from its original blood supply in areas like the back or abdomen.
Using a technique called microsurgery, the surgeon attaches the blood vessels from the tissue to new blood vessels in the chest area. This method provides the reconstructed breast with a new blood supply, promoting integration of the tissue. Free flaps offer flexibility in shaping and positioning the new breast mound.
Locations of Donor Tissue
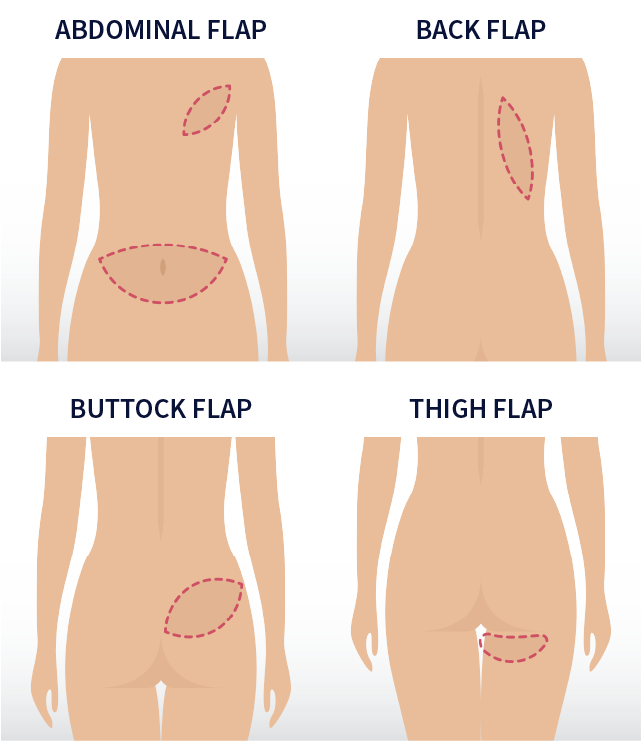
The location of the donor tissue used in flap surgery varies in breast flap reconstructions. These procedures are classified based on the site from which the tissue is obtained: abdomen, back, buttock and thigh. Each donor site offers unique benefits and considerations for patients.
Abdominal Flaps
Abdominal flaps use tissue from the stomach area for breast reconstruction. Often, the abdomen provides enough tissue so that breast implants are not needed. The specific techniques vary based on how the tissue is transferred and whether abdominal wall muscles are used. The donor site often resembles a “tummy tuck.” However, some techniques may reduce abdominal muscle strength and potentially cause bulging. This option may not be suitable for very thin patients or those who have had a previous tummy tuck procedure.
Back Flaps (Latissimus Flap)
Back flaps, particularly the latissimus dorsi flap, involve moving muscle, fat, skin and blood vessels from the upper back to the chest. Because less tissue is available compared to an abdominal flap, this method often (although not always) requires a breast implant to achieve the desired volume. The tissue is tunneled under the skin to the front of the chest.
Latissimus dorsi flaps can cause shoulder weakness, especially when the patient moves her arm above 90 degrees and inward while rotating her shoulder. For that reason, some patients may choose to have a partial latissimus flap, also called a thoracodorsal artery perforator (TDAP) flap.
Buttock Flaps (Gluteal Flap)
Buttock flaps, also known as gluteal free flaps or gluteal artery perforator (GAP) flaps, use tissue from the buttocks to create a new breast. This option is suitable for patients who are unable to use abdominal tissue due to thinness, previous surgeries or other reasons.
During the procedure, skin, fat and blood vessels are removed from the buttocks and transplanted to the chest without removing any muscle. The blood vessels are reattached using microsurgery. However, this technique may change the contour of the buttocks, causing issues like skin dimpling, which has limited its popularity.
Thigh Flaps
Thigh flaps are a viable option for breast reconstruction when abdominal tissue is not suitable. Depending on the patient’s preferences and body build, tissue may be harvested from the inner or outer thighs. These procedures involve microsurgery to reconnect blood vessels in the chest. Typically, thigh flaps provide enough tissue for small to medium-sized breasts. In some cases, tissue from both thighs may be used to reconstruct a single breast, offering a flexible solution for patients needing alternative donor sites.
Rib-Sparing Reconstruction
In some types of flap surgery, all or part of a rib may need to be removed to access the needed blood vessels.
Rib-sparing surgery is a technique used in certain types of breast reconstruction where the rib is preserved to avoid additional trauma and complications. The surgeon uses specialized techniques to work around the ribs rather than removing or cutting them. This approach minimizes changes to the chest wall, potentially reducing postsurgery pain.
Abdominal Perforator Exchange (APEX) Flap
This is a form of free flap breast reconstruction surgery that uses skin and fat from the lower abdomen to create a new breast. It is nearly the same as deep inferior epigastric perforator (DIEP) surgery, only differing in the technique the surgeon uses to separate the flap from the muscle.
Deep Inferior Epigastric Perforator (DIEP) Free Flap
During a DIEP free flap surgery, fat and skin are removed from the lower abdomen and reconnected to the chest with microsurgery. No muscle is moved, so there is less chance of bulging or weakness at the donor site after surgery.
Free Muscle-Sparing Transverse Rectus Abdominis Muscle (MS-TRAM) Flap
This surgery moves a portion of the transverse rectus abdominus muscle from the lower abdomen to the chest. The advantage of this procedure is that the donor site is less likely to bulge or weaken after surgery.
Gluteal Artery Perforator (GAP) Flap
The gluteal free flap or gluteal artery perforator (GAP) flap is a possible option for patients who are unable or do not wish to use a lower abdominal donor site. It requires expert surgical center experience. This surgery uses tissue (but not muscle) from the buttocks to create a new breast. When the artery from the upper buttocks is used, the procedure is called a superior gluteal artery perforator (SGAP) flap. When the artery from the bottom of the buttocks is used, it becomes an inferior gluteal artery perforator flap (IGAP).
Lateral Thigh Perforator (LTP) Flap
Patients who have more fatty tissue on the outer thigh and who are not candidates for a DIEP flap may want to consider the LTP flap. This surgery relocates fat and skin tissue from the “saddlebag” area of the thigh to the breast without moving any muscle.
Latissimus Dorsi Flap
The latissimus dorsi flap is the most common type of pedicle flap used in breast reconstruction. In this surgery, skin, muscle and fat from the back are brought around to the chest to make a new breast mound. This reconstructive surgery is sometimes combined with an implant since there is typically less tissue on the back versus the abdomen.
Lumbar Artery Perforator (LAP) Free Flap
The LAP flap is a newer free flap procedure sometimes used when the patient does not have enough abdominal tissue to use as a donor site. In this surgery, skin, fat and blood vessels are taken from the “love handle” area of the lower back. The flap is then reconnected at the chest.
Profunda Artery Perforator (PAP) Flap
This is a free flap surgery that takes skin and fat from the patient’s inner thigh to create a new breast flap.
This method of reconstruction has been gaining in popularity because it does not involve cutting or moving muscle, and the blood vessels are typically easier to work with.
Superficial Inferior Epigastric Artery (SIEA) Free Flap
This is another free flap surgery that uses the lower abdomen as a donor site. SIEA uses skin, fat and blood vessels to craft a new breast in a similar way as DIEP or TRAM free flap surgery. However, different blood vessels are used. This surgery is uncommon because not every patient has these blood vessels.
Thoracodorsal Artery Perforator (TDAP) Flap
This is another type of pedicle flap taken from the back. Skin and fat from the upper back are used to form the new breast. No muscle is transferred. This type of reconstruction is typically used when the patient has only had a lumpectomy or partial mastectomy.
Transverse Upper Gracilis (TUG) Flap
In this surgery, skin, fat and part of the gracilis muscle of the inner thigh are used to make a free flap for a new breast. Many times, the thighs only provide enough tissue to make a small or medium breast, but sometimes a flap may be taken from each thigh and combined to form one breast.
Agency for Healthcare Research and Quality. Breast reconstruction after mastectomy: a systematic review and meta-analysis, July 2021.
https://www.ncbi.nlm.nih.gov/books/NBK572806/American Cancer Society. Breast reconstruction using your own tissue (flap procedures), October 20, 2021.
https://www.cancer.org/cancer/types/breast-cancer/reconstruction-surgery/breast-reconstruction-options/breast-reconstruction-using-your-own-tissues-flap-procedures.htmlNational Cancer Institute. Breast reconstruction after mastectomy, February 24, 2017.
https://www.cancer.gov/types/breast/reconstruction-fact-sheetBamba R, Hanson SE, Beederman M, Garza RM, Chang DW. To spare or not to spare rib: A survey on internal mammary vessel preparation in microsurgical breast reconstruction. Microsurgery. November 2022.
PMID: 36172931DellaCroce FJ, DellaCroce HC, Blum CA, Sullivan SK, Trahan CG, Whitten Wise M, Brates, IG. Myth-busting the DIEP flap and an introduction to the abdominal perforator exchange (APEX) breast reconstruction technique: a single-surgeon retrospective review. Plast Reconstr Surg. April 2019.
PMID: 30730497