Melanoma Treatment & Survival Rate
April 2, 2026
This page was reviewed under our medical and editorial policy by Gaurav Singh, M.D., M.P.H., F.A.C.M.S., Mohs Micrographic Surgeon and Dermatologist, City of Hope® Cancer Center Chicago.
Treatment options for melanoma depend on various factors, especially the stage and location of the cancer. While early-stage melanomas are often treated with surgery alone, more advanced cancers frequently require other treatments, such as immunotherapy or targeted therapy, or combination treatments. The care team also considers the risk of recurrence, whether the cancer cells have certain genetic mutations and the patient’s overall health when personalizing the treatment plan.
Who Treats Melanoma?
Speed to experts who specialize in treating the patient’s particular type of melanoma matters. The team may include the following multidisciplinary providers and others:
- A dermatologist, who specializes in diagnosing and treating diseases affecting the skin
- A Mohs surgeon, who is equipped with tools as the surgeon and pathologist to offer the best cure rates with the smallest possible scarring
- A surgical oncologist, who performs a range of surgical techniques to remove cancer
- A medical oncologist, who treats cancer with drugs such as chemotherapy, immunotherapy or targeted therapy
- A radiation oncologist, who uses high-energy beams of radiation to destroy cancerous tissue
- A pathologist, who examines tissue samples for diagnostic purposes to help determine a treatment plan
- A radiologist, who utilizes imaging tools and interventional techniques to diagnose and treat cancer
- Supportive care providers, who focus on cancer- and treatment-related side effects and symptom management
Melanoma Treatments
Treatment options for melanoma are rapidly evolving. While surgery is the most common treatment for all stages of melanoma, systemic treatments like immunotherapy and targeted therapy have unlocked new options, especially for patients with advanced disease.
Researchers also continue to investigate new therapies and combinations of treatment for melanoma, including vaccine therapy, which uses a substance that stimulates the immune system to locate and destroy cancer cells. Vaccine therapy is currently being tested in clinical trials for Stage 3 melanoma that can’t be removed by surgery.
Melanoma Surgery
Regardless of stage, surgery is the first treatment for most patients with melanoma — and for those with early-stage disease, surgery may be the only treatment needed.
In cases where melanoma is confined to the skin, a surgeon’s goal is to remove all traceable cancer. When melanoma is more advanced, surgery may be more complex. The surgical options differ depending on the treatment goals.
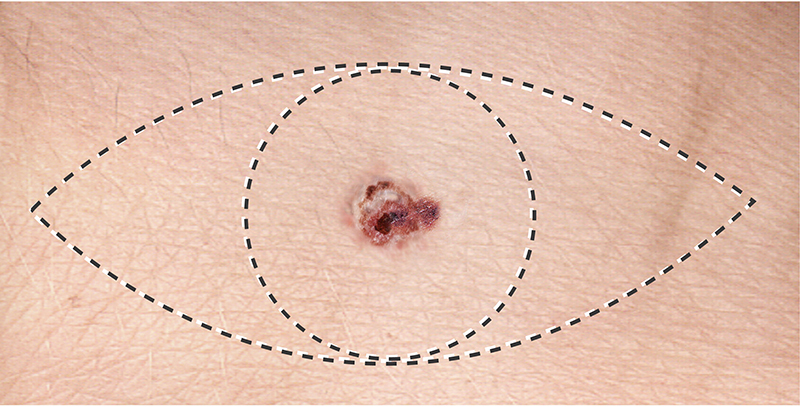
Wide local excision: A wide local excision is the standard surgical treatment used to remove melanoma. During this procedure, the surgeon removes the tumor in addition to some surrounding normal tissue called the margins, which are wider because the diagnosis is already known.
Mohs surgery: A tissue-sparing technique called Mohs surgery is a likely option for patients with non-melanoma skin cancer or early-stage melanoma on the face or other sensitive areas. During this outpatient procedure, the dermatologist or surgeon removes a single disc of skin and then examines it under a microscope for cancer cells before moving to the next layer. Mohs surgery is routinely used to treat melanoma in situ (stage 0) or lentigo maligna melanoma, a subtype of melanoma that usually occurs on sun-damaged skin.
Lymph node dissection: When a biopsy shows that lymph nodes near the melanoma contain cancer cells, a lymph node dissection or lymphadenectomy is likely to follow. All lymph nodes in a particular region are removed during this procedure.
While surgery can be scary, building a trusted relationship with your surgeon can help ease fears and increase confidence in the outcomes. “I emphasize developing a deeply human-centered approach to aligning cancer treatment with patient preferences,” says Gaurav Singh, M.D., M.P.H., F.A.C.M.S., Mohs micrographic surgeon and dermatologist at City of Hope® Cancer Center Chicago. “It starts with building a relationship first by meeting not just the patient, but also their family and friends.
“Shared decision-making is also critical,” he adds. “Rather than presenting a plan and asking for compliance, I facilitate a conversation, discussing the latest evidence and treatment options collaboratively, so patients feel empowered as active participants in their own care and not passive recipients of it.”
Radiation Therapy
Radiation therapy uses high-energy rays to destroy cancer cells and shrink tumors with precision. Though not commonly used to treat melanoma, radiation therapy is involved when:
- Surgery is not a good option, for example, if the melanoma has spread toward, but not as far as, the lymph nodes.
- Melanoma isn’t completely removed by surgery.
- Lymph nodes have been removed, but the cancer is at high risk of returning.
- Melanoma returns and begins growing again on the skin or in lymph nodes.
- Pain or other symptoms can be relieved by radiation therapy.
- Melanoma has spread to the brain or spinal cord.
Types of Radiation Therapy for Melanoma
Radiation therapy options for patients with melanoma include:
External beam radiation therapy (EBRT), which is primarily used to treat melanoma, targets radiation from a source outside the body on the cancer.
Stereotactic radiosurgery (SRS), which is sometimes used for melanoma that has spread to the brain. During one or more appointments, a radiation oncologist directs high doses of radiation precisely at the tumor(s).
Stereotactic body radiation therapy (SBRT), which is a technique similar to SRS. It requires a linear accelerator — a machine that creates radiation — but is used to treat tumors in other areas of the body, such as the lungs or spine.
Chemotherapy
Medical oncologists may consider chemotherapy for patients with advanced melanoma, if the cancer hasn’t responded to other treatments. These drugs aren’t typically used as first-line treatments because targeted therapy and immunotherapy are usually more effective.
Chemotherapy can shrink tumors, but its impact on survival is unclear. Side effects from chemo include hair loss, nausea and vomiting, mouth sores, loss of appetite, diarrhea or constipation, increased risk of infection, fatigue and easy bruising or bleeding.
Chemotherapy Options for Melanoma
Various chemotherapies — administered via IV or pill alone or in combination — can be used to treat melanoma. Oncologists dose chemo in cycles, which generally last for a few weeks, followed by a rest period for recovery.
The most common drugs include:
- Dacarbazine (DTIC)
- Temozolomide
- Nab-paclitaxel
- Paclitaxel
- Cisplatin
- Carboplatin
If melanoma returns near its original site in an arm or leg, the patient may receive regional chemotherapy — known as isolated limb infusion (ILI) or Isolate limb perfusion (ILP) — which delivers the drug only to that limb, typically causing fewer side effects.
- For ILI, long tubes are inserted through the skin into the artery and vein. This simpler, quicker method often doesn’t need general anesthesia.
- For ILP, the artery and vein are surgically isolated from the body's circulation and then connected to tubes that lead to a machine in the operating room.
Immunotherapy
Among the most promising treatments for advanced melanoma is immunotherapy — drugs that help stimulate the immune system to recognize and kill cancer cells.
Types of Immunotherapy for Melanoma
The care team will select the type of immunotherapy based on a variety of factors. Talk to the care team about the patient’s immunotherapy treatment options.
Immune checkpoint Inhibitors: To help the immune system guard itself from attacking normal cells, it uses “checkpoint” proteins, which act like on/off switches. They turn on to kill cancerous cells and turn off to avoid damaging normal cells. Following are immune checkpoint inhibitors that target these checkpoints.
- PD-1 inhibitors: Pembrolizumab (Keytruda) and nivolumab (Opdivo) block the PD-1 protein on T cells, strengthening the immune response against melanoma. They are given intravenously, usually every two to six weeks.
- PD-L1 inhibitor: Atezolizumab (Tecentriq) is a drug that blocks PD-L1, boosting the immune response against melanoma cells. It can be combined with cobimetinib and vemurafenib for melanomas with a BRAF gene mutation that are inoperable or have spread. The drug is administered via IV every two to four weeks, or as an injection every three weeks.
- CTLA-4 inhibitor: Ipilimumab (Yervoy) is a checkpoint inhibitor that blocks CTLA-4, a T cell protein that regulates immune responses. It treats melanomas that can't be surgically removed or have spread, and may also be used after surgery as adjuvant therapy to reduce recurrence risk. Ipilimumab alone is less effective and has more serious side effects than PD-1 inhibitors. It’s given intravenously every three weeks for four doses.
- LAG-3 inhibitor: Relatlimab targets LAG-3, a checkpoint protein that regulates immune responses. Used with the PD-1 inhibitor nivolumab as Opdualag, it treats advanced or inoperable melanoma. The drug is delivered via IV infusion every four weeks.
Some common side effects can accompany immune checkpoint inhibitors, including fatigue, cough, nausea, poor appetite, diarrhea, constipation, joint pain and skin rash.
Interleukin-2: Interleukins are proteins that stimulate the immune system. Lab-made interleukin-2 (IL-2), such as aldesleukin, is sometimes used to treat melanoma. High-dose IL-2 can shrink some advanced melanomas if other treatments, like immune checkpoint inhibitors, no longer work. It’s typically given intravenously, with possible side effects, including flu-like symptoms, low blood counts, and, at high doses, serious fluid buildup.
Tumor-infiltrating lymphocyte (TIL) therapy: TILs are T cells from the immune system that enter tumors to fight cancer. Lifileucel (Amtagvi) is a TIL therapy for advanced melanoma after other treatments have failed. The process involves surgically removing a tumor, isolating and multiplying TILs in a lab, then infusing them back into the patient through an IV. Patients receive chemotherapy beforehand to help their bodies accept the TILs, followed by IL-2 to boost the immune response.
TIL therapy must be done in a hospital due to its risk of serious side effects, such as very low blood cell counts, heart problems and internal bleedings.
Oncolytic virus therapy: Viruses can infect and destroy cells, and some are modified in labs to target cancer cells — these are known as oncolytic viruses. They not only kill cancer cells but also stimulate the immune system against them.
Talimogene laherparepvec (Imlygic), or T-VEC, is an oncolytic virus used for melanomas in the skin or lymph nodes that can’t be surgically removed. It’s injected into tumors every two weeks, which can shrink both treated and untreated tumors. Potential side effects include flu-like symptoms and injection site pain.
BCG vaccine: The Bacille Calmette-Guerin (BCG) vaccine uses a germ similar to the one causing tuberculosis. While it doesn’t cause serious illness, it stimulates the immune system. Though rarely used today, BCG may be injected into tumors to help treat stage 3 melanomas.
Imiquimod cream: Imiquimod (Zyclara) — a topical medication applied as a cream — activates a local immune response against skin cancer cells. For early stage (stage 0) melanomas in sensitive facial areas, imiquimod may be used if surgery can’t entirely remove the tumor. Imiquimod may also be considered for certain melanomas that have spread on the skin, particularly when surgery can’t be done. The cream is typically administered two to five times a week for three months. Some patients experience significant skin reactions or flu-like symptoms during treatment.
Targeted Therapy
As its name suggests, targeted therapy targets melanoma cells rather than broadly killing all rapidly dividing cells as chemotherapy does. These drugs may be effective in treating advanced melanomas when specific gene changes (mutations) are identified in the cancer cells.
If melanoma spreads beyond its original location, a biopsy sample is often analyzed to determine whether these gene changes are present, a process referred to as biomarker testing.
Types of Targeted Therapy for Melanoma
About half of melanomas have mutations in the BRAF gene, causing altered BRAF proteins that promote tumor growth. BRAF and MEK inhibitors can be beneficial treatments for these cases but typically don’t work on melanomas with normal BRAF genes.
BRAF inhibitors: Used for advanced or inoperable melanoma, BRAF inhibitors Vemurafenib (Zelboraf), dabrafenib (Tafinlar) and encorafenib (Braftovi) directly target BRAF mutations.
Dabrafenib, coupled with the MEK inhibitor trametinib, is also given after surgery in people with stage 3 melanoma to lower recurrence risk. These drugs are taken as pills or capsules once or twice daily, with common side effects including skin thickening, itching, rash, sun sensitivity, fever, joint pain, headache, fatigue, nausea and hair loss.
MEK inhibitors: The MEK inhibitors trametinib (Mekinist), cobimetinib (Cotellic) and binimetinib (Mektovi) target MEK proteins and may also treat melanomas with BRAF changes. Taken orally once or twice daily, these drugs are used for melanoma that has spread or can’t be fully removed. Trametinib is also combined with dabrafenib after surgery for stage 3 melanoma to lower recurrence risk.
A MEK inhibitor is most often combined with a BRAF inhibitor, resulting in longer-lasting tumor shrinkage and fewer specific side effects compared to using either drug alone. Common side effects include rash, swelling, nausea, diarrhea and sunlight sensitivity. Rare but serious risks are heart, lung or liver damage; bleeding or clots; vision or muscle problems; and infections.
Other gene changes: A small percentage of melanomas have changes in the C-KIT gene, especially those that appear on the palms, soles, under nails (acral melanomas), mucosal areas or areas with chronic sun exposure. Targeted drugs like imatinib (Gleevec) and nilotinib (Tasigna) may be effective if these changes are found. The care team may test for C-KIT mutations in advanced melanoma from these locations.
Oncologists may also test for other less common gene changes in NRAS, ALK, ROS1 or NTRK genes. If present, specific targeted therapies may be an option.
Melanoma Survival Rate
When discussing survival rates, it’s important to consider the type, size, thickness, location and stage of melanoma in addition to the patient’s overall health. Advancements in precision melanoma treatments, including immunotherapy and targeted therapy, are positively impacting outcomes — and, if detected in the early stages, the five-year relative survival rate for melanoma is 99%.
The National Cancer Institute’s Surveillance, Epidemiology and End Results (SEER) database tracks five-year relative survival rates for melanoma. This describes how long someone is alive five years after diagnosis, compared to someone without that cancer type. SEER uses localized, regional and distant stages, meaning:
Localized: No sign that cancer has spread beyond the skin where it started.
Regional: Cancer has spread beyond the skin to nearby structures or lymph nodes.
Distant: Cancer has spread to distant parts of the body, such as the lungs, liver, skin or distant lymph nodes.
The following numbers are based on people diagnosed with melanoma between 2015 and 2021:
| SEER stage | Five-year relative survival rate |
|---|---|
| Localized | 100% |
| Regional | 75.7% |
| Distant | 34.6% |
Melanoma Treatment at City of Hope
City of Hope’s approach to treating melanoma starts with a coordinated, multidisciplinary care team. We strive to offer patients the most individualized treatment plan that includes the newest therapies and innovative treatment combinations effective for even the most advanced melanomas.
We treat patients at all stages of disease, from initial diagnosis to advanced stages, including those with recurrent disease or metastatic melanoma.
“We emphasize understanding the whole patient and using compassion as a clinical tool, not a soft add-on,” Dr. Singh says. “It’s about treating personalized medicine as both a scientific and deeply interpersonal practice. This setting is where the best treatment plan is one the patient genuinely understands, agrees with, and feels seen in.”
- National Cancer Institute. Melanoma treatment (PDQ®)–patient version, May 16, 2025. https://www.cancer.gov/types/skin/patient/melanoma-treatment-pdq
- American Cancer Society. Treating melanoma skin cancer, October 27, 2023. https://www.cancer.org/cancer/types/melanoma-skin-cancer/treating.html
- Melanoma Research Alliance. Treatment options,
https://www.curemelanoma.org/patient-eng/melanoma-treatment - National Cancer Institute Surveillance, Epidemiology, and End Results Program. Cancer stat facts: melanoma of the skin. https://seer.cancer.gov/statfacts/html/melan.html